Gastrointestinal cancer(Colorectal cancer)
- HOME
- Cancer(View by Body Part)
- Gastrointestinal cancer(Colorectal cancer)
- Endoscopic surgeon with God’s hands has a keen sense to detect dangerous colorectal cancer
Endoscopic surgeon with God’s hands has a keen sense to detect dangerous colorectal cancer
23.10.18
What dangerous colon cancer has Professor Kudo discovered?
It is believed that all colorectal cancer occurs from polyps, but I was the first to find the depressed type, which occurs as cancer from the beginning. However, we were the first in the world to discover the depressed type of cancer that develops as a cancer from the beginning and infiltrates into colon rather than in the form of polyps, like stomach and esophageal cancer.
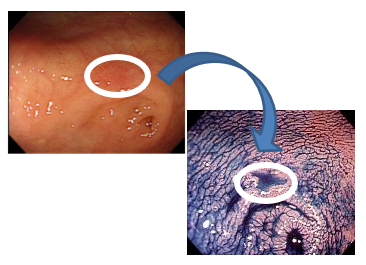
This is an endoscopic image of the colon with normal mucosa, where there is a very slight redness (surrounded by a white circle). No one could tell that this was cancer, but when a dye called indigo carmine was applied to the area, it could be seen that the area was depressed (indented). Moreover, the edge of this margin width is a bit jagged. This is the shape of both gastric and esophageal cancer which is very characteristic configuration of cancer.
Why are depressed forms so dangerous?
While the cancer remains in the colon, it is not a problem, but if it infiltrates blood vessels or lymph vessels, metastasizes to the lungs or liver, and grows larger and larger at the metastatic site, digestion and respiratory functions will be impaired, leading to death very quickly. The speed of progression of the depressed type is 10 to 20 times (!) faster than that of polyps. It is fast, progressing quickly in about one year.
The number of colonoscopies seems to be declining due to the Covid-19 pandemic, and the mortality rate for colorectal cancer only tends to increase abnormally because of this. Not performing examinations is fatal.
We were the first in the world to demonstrate that this slight redness could be clearly identified as a depression by applying a dye to it, and we presented it around the world.

Who is at risk for colorectal cancer? When should people begin examination?
If someone in your family has had colorectal cancer, you should consider your genetic risk of colorectal cancer. I recommend that the patient be examined once at cancer age (around age 20). Recently, we have seen an increase in the number of younger patients, especially women. People who are inactive or constipated should take note. Stools contain slight amounts of carcinogens, and the fact that they are in the intestines for an extended period of time means that there is a risk of cancerous growth of the mucous
Please tell me about the examination!
Screening of colorectal cancer requires endoscopy which has much higher diagnostic accuracy than X-rays.
With an endoscope, you can distinguish the difference in color, light redness, and if you apply dye to it, you will see a depression. If you look at it with a camera magnified to 100x or 520x, which we developed in a tie-up with Olympus, you can see the cells, even the nucleus.
Cancer is immediately recognizable as “cancer” just by looking at the size of the nucleus, because the nucleus is enlarging.
It is no wonder that endoscopy specialists from Japan and abroad have come to you to learn from you personally during his “Kudo Pilgrimage.”
At the time I moved from Niigata University to Akita Red Cross Hospital in my hometown of Akita, I was also a surgeon. Before a surgical operation, we would not perform endoscopies on other organs, but in the case of the colon, we could not perform surgery without first collecting tissue for examination by endoscopy, so we did a lot of endoscopies in the surgery department. Many inspections that I practiced led to the detection of the depressed type.
Later, I was invited by Showa University Hospital to teach as a professor of both gastroenterology and gastroenterological surgery. I am now the oldest professor, but I am getting better and better! Doctors from all over the world came to study at Showa University to learn a lot of things about endoscopic techniques. Doctors who returned to their home countries and my students whom I sent abroad are now active all over the world, including one who became a professor at the University of Oslo in Norway, another at the Mayo Clinic in the United States, and another who was invited many times by the University of London in England and later became a professor.
What happens if the examination shows cancer?
If it is less than 1 cm, I try to see if it rises by adding saline solution on the spot. If it gets raised, then cut off the raised area, and that’s (the end of) the treatment. Therefore, if it is about 1 cm, it is very likely that it can be cured by endoscopic treatment.
Patients from overseas who wish to undergo examination and treatment
We accept examination and treatment from patients in Japan, overseas, and from all over the world. I think it is our mission to provide the best examination and optimal treatment. Please come to our clinic.

About Tokyo Endoscopic Clinic
The clinic is located in front of Shinjuku Station in Tokyo and specializes in colonoscopy and upper gastrointestinal endoscopy.
If a patient wishes to have an upper and lower endoscopy at the same time, it can be performed in about 10 minutes in addition to the colonoscopy.
Examinations on weekends are also available.
If polyps are found during endoscopy, and if they are 2 cm or smaller, they can be removed by endoscopy during the examination. If it is over 2 cm, we will refer you to a partner medical institution such as a university hospital.
Please tell us the features of your facilities
We have state-of-the-art endoscopic equipment. One of the major features of the clinic is the magnifying endoscope, an instrument that can diagnose polyps up to 100x-520x, making it possible to instantly diagnose whether the polyp is benign or malignant, and to provide treatment appropriate to the situation, which is one of the clinic’s strengths.
This magnifying endoscope was developed by Professor Shinei Kudo, who is a special advisor to our clinic.